A 69-year-old male patient attended complaining of discomfort caused by repeated accumulation of food matter in sector 4.
Clinical examination revealed that teeth 45 and 46 had been reconstituted using two amalgams located in the occluso-distal and the mesio-occluso-vestibular respectively. Tooth 47 bears a ceramic-metallic crown. All the teeth showed a negative response to the percussion and palpation tests, Pulp vitality was positive for teeth 45 and 46.

In tooth 46, a slight break of the amalgam was observed in mesial; this, following verification of all the contact points, appears to explain why the patient came for an appointment.
Several flaws or cracks were also noted in this tooth; this is not unusual when this type of reconstitution is present.
The bite test, however, remained negative.

An X-ray examination revealed resumption of decay under the amalgams in teeth 45 and 46. The fit of the ceramic-metallic crown no longer seems radiologically tight. After discussion with the patient, it was decided to replace the amalgam in 45 with a composite resin, using the direct technique, and to restore 46 using an indirect partial bonded restoration in order to respect the therapeutic gradient. The patient deferred the repair work to 47 for financial reasons.

On the day of preparation, the surgical site was set up at the beginning of the treatment in order to withdraw the amalgams safely.
The dam also protected the exposed dentine against saliva and facilitated a visual examination of the tooth.
It should be noted that the shade was determined before the field was set up, in order to avoid errors connected with tooth dehydration.

After removal of the two amalgams and the decayed tissue, the occluso-distal composite for 45 was made. For 46, in view of the weakness of the remaining walls and the presence of numerous cracks, a partial bonded restoration with total overlay was decided upon, and work to prepare this was commenced.
The design of the preparation was optimised using a composite material, according to the principle of CDO (Cavity Design Optimisation). A classic bonding procedure was therefore performed.
The last photo-polymerisation of the composite was carried out using glycerine gel which covered the preparation, to avoid the presence of a non-polymerised surface layer caused by the inhibiting action of oxygen.

The dental dam was removed in order to provide the finishes. It is important to ensure that the enamel margins, essential for adhesion, are not covered with any excess of composite resin.

The double-mixture print was provided using silicone; the antagonist used alginate. The whole was then sent to the prosthesis laboratory.

A temporary overlay using isocasting was produced in order to ensure dimensional stability while the prosthesis was being designed.

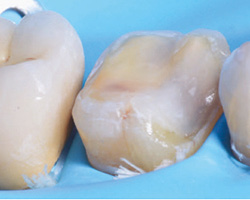
The impression was cast and the model scanned in the prosthesis laboratory. The piece was then designed and machined using a pre-polymerised hybrid ceramic disc Numerys HC, consisting of 75% ceramic and 25% resin. Finally, it was coloured and checked by the prosthetist.

The overlay was once again checked in the office against the working model and double (contact points and fit).

The prosthesis, after decontamination, was tried in the mouth before and after application of the field to ensure that the field did not interfere on insertion.
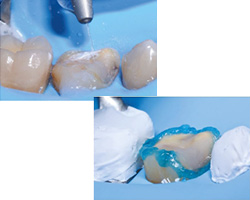
The clinical procedure of bonding could then begin and required the application of a strict protocol which began with treatment of the surface of the tooth. Gentle sanding with alumina for 5 seconds, plus etching of the enamel using Dentoetch (37% orthophosphoric acid) for 30 seconds, were carried out in order to increase the bonding capacity of the surface.
The internal surface of the prosthesis must also undergo surface treatment. To achieve this, it was also sanded using alumina for5 seconds. After that, Silan-It was applied, dried and left in the ambient air for one minute to make the piece more easily wettable. Finally, the same adhesive was applied to the piece and blown, also to allow good spreading.

Assembly was carried out using a dual adhesive Total C-Ram; Some of the excess was removed before polymerisation, using a pincer impregnated with a modelling fluid for composite. The piece was then photo-polymerised for 20 seconds per face. The remaining excess was then removed using the scalpel blade.

The dam was removed and the finishes applied using polishers for composite.

The occlusion was then verified in static and dynamic, in order to ensure that the prosthetic piece fitted perfectly into the patient’s occlusal diagram.

A post-operative X-ray was performed in order to ensure that the restoration was suitable and there was no excess adhesive in the embrasures.